Culture makes the country prosperous and the nation strong. Without a high degree of cultural self-confidence and cultural prosperity, there would be no great rejuvenation of the Chinese nation. Building a strong socialist culture is an important task of building a strong socialist modernization country. How to understand the rich connotation of Socialism with Chinese characteristics culture? How to vigorously build a socialist cultural power in the new era? Several articles in this observation edition focus on these issues.
— — Editor
The core of building a cultural power is to develop Socialism with Chinese characteristics culture (People’s Watch)
She Shuanghao
Culture is the spiritual achievement accumulated by a country and a nation in the long-term development history, and it is the spiritual lifeline that keeps the country and the nation alive and the spiritual home of the people. In contemporary China, the core of building a socialist cultural power is to develop Socialism with Chinese characteristics culture and constantly create new glories of Chinese culture. Socialism with Chinese characteristics culture is the spiritual force to promote the development of Socialism with Chinese characteristics. The report of the 19th National Congress of the Communist Party of China pointed out: "Socialism with Chinese characteristics culture originated from the excellent traditional Chinese culture nurtured by the 5,000-year-old civilization history of the Chinese nation, and was cast in the revolutionary culture and advanced socialist culture created by the party leading the people in revolution, construction and reform, and rooted in the great practice of Socialism with Chinese characteristics." This important thesis scientifically defines Socialism with Chinese characteristics culture and profoundly reveals the essential attribute of Socialism with Chinese characteristics culture. To build a strong socialist cultural country, we need to understand and grasp Socialism with Chinese characteristics culture from multiple dimensions.
Socialism with Chinese characteristics culture highlights China characteristics.
Socialism with Chinese characteristics culture is the culture of China, with strong China characteristics, China style and China style. Its value subject is the people of the Communist Party of China (CPC) and China, its cultural content is the spiritual achievement created by the Communist Party of China (CPC) and the Chinese people, and it has a clear Chinese position. To develop Socialism with Chinese characteristics’s culture and build a socialist cultural power, we should highlight the characteristics of China and reflect the cultural ideas of the people of the Communist Party of China (CPC) and China.
Every culture has its own roots, and the roots of Socialism with Chinese characteristics culture are the excellent traditional Chinese culture nurtured by the Chinese nation in its history of more than 5,000 years. This is the gene of Socialism with Chinese characteristics culture, the fertile soil for nourishing Socialism with Chinese characteristics culture, and the characteristic and advantage of Socialism with Chinese characteristics culture. Chinese culture is the only uninterrupted ancient culture in the world. It has developed tenaciously with strong vitality for thousands of years, creating one glory after another in the history of human civilization. The Communist Party of China (CPC) is the inheritor and promoter of Chinese excellent traditional culture, and has always attached great importance to the role of Chinese excellent traditional culture. To build a strong socialist culture, we must actively activate the excellent Chinese traditional culture and make it the internal nourishment for the development of Socialism with Chinese characteristics culture. To achieve this, we need to attach great importance to the creative transformation and innovative development of Chinese excellent traditional culture. Socialism with Chinese characteristics culture was created by the Party leading the people in revolution, construction and reform, and rooted in the great practice of Socialism with Chinese characteristics. Socialism with Chinese characteristics culture is the embodiment of Socialism with Chinese characteristics Road, Socialism with Chinese characteristics Theory System and Socialism with Chinese characteristics System at the cultural level, showing the spirit of China, the value of China and the strength of China, and reflecting the ideological concept and moral norms of contemporary Chinese. This determines that the development of Socialism with Chinese characteristics culture must abandon the kind of "respecting foreign countries" and "taking foreign countries as beauty"The wrong concept of "only following the foreign countries".
Socialism with Chinese characteristics culture highlights the essence of socialism.
Socialism with Chinese characteristics culture is a socialist culture, not a culture of other natures, which is inherent in the cultural nature. Socialist culture is a more advanced cultural form than capitalist culture and feudal culture. To develop Socialism with Chinese characteristics culture and build a socialist cultural power, we must firmly grasp the essential attributes of socialism and constantly strengthen our cultural self-confidence.
Socialism with Chinese characteristics culture is cast in the revolutionary culture and advanced socialist culture created by the Party leading the people in revolution, construction and reform. Both revolutionary culture and advanced socialist culture belong to socialist culture, which is the spiritual achievement that the Communist Party of China (CPC) led the people of China to form and accumulate in the practice of revolution, construction and reform. At the same time, after creative transformation and innovative development, Chinese excellent traditional culture is also adapted to Socialism with Chinese characteristics. The nature of socialism determines that Socialism with Chinese characteristics culture always insists on serving the people and socialism, and it is a people-centered culture. The reason why Socialism with Chinese characteristics culture has always maintained its socialist nature is that it always adheres to the guidance of Marxism and represents the direction of advanced human culture. Therefore, to develop Socialism with Chinese characteristics culture and build a socialist cultural power, we must always adhere to the guidance of Marxism, which is the fundamental sign that Socialism with Chinese characteristics culture is different from other cultures. Without the guidance of Marxism and the nature of socialism, even if more cultural products are produced, it cannot be said that a socialist cultural power has been built.
Socialism with Chinese characteristics culture has practical spirit.
Socialism with Chinese characteristics culture is a vivid reflection of Socialism with Chinese characteristics’s great practice, and it is also the spiritual driving force to promote Socialism with Chinese characteristics’s great practice. According to the basic viewpoint of Marxism, social existence determines social consciousness, and social consciousness reacts on social existence. As a social consciousness, culture is a reflection of social existence in the final analysis. Socialism with Chinese characteristics culture, as a concept and spiritual thing, is in the final analysis a reflection of Socialism with Chinese characteristics’s great practice, which in turn reacts to Socialism with Chinese characteristics’s great practice. To develop Socialism with Chinese characteristics’s culture and build a socialist cultural power, we must firmly grasp its practical spirit, so that spiritual civilization and material civilization can develop in harmony.
Since the 18th National Congress of the Communist Party of China, with great political courage and strong responsibility, the CPC Central Committee with the Supreme Leader as the core has solved many problems that have been tried for a long time but not solved, and accomplished many major events that were tried but not done in the past, which has promoted historic changes in the cause of the party and the country, and the Chinese nation has ushered in a great leap from being rich to being strong. It is in the great development of Socialism with Chinese characteristics’s career that Socialism with Chinese characteristics culture has ushered in great development and prosperity; The great development and prosperity of Socialism with Chinese characteristics culture has promoted the great development of Socialism with Chinese characteristics. In the new era, to develop Socialism with Chinese characteristics’s culture and build a socialist cultural power, we should obtain a steady stream of power for cultural development from practice, and at the same time make cultural development an inexhaustible spiritual power for reform and development.
(The author is Dean of School of Marxism, Wuhan University, and a researcher at Socialism with Chinese characteristics Theoretical System Research Center, Hubei Province.)
Three Relationships Should Be Handled Scientifically in Building a Powerful Cultural Country (All Written by Everyone)
He xingliang
Building a strong socialist culture is the foothold of promoting the prosperity of socialist culture and the inherent requirement of realizing the great rejuvenation of the Chinese nation. To build a strong socialist cultural country, we need to deal with three kinds of relations in practice.
The first is the relationship between inheritance and innovation. Inheriting Chinese excellent traditional culture is the consensus of all walks of life at present. If the culture of a country or nation loses its tradition, it may become a vassal of other cultures, and it is impossible to have a position in the world. Many contents in Chinese excellent traditional culture have high scientific value, historical value and artistic value, and are the crystallization of Chinese wisdom for thousands of years. At present, the key to inheriting Chinese excellent traditional culture is to inherit and carry forward its rich and excellent philosophical thoughts, humanistic spirit, enlightenment thoughts and moral concepts. These are the soul and essence of Chinese excellent traditional culture, which have eternal value and have been handed down from generation to generation in history. In addition, we should inherit all kinds of excellent literary works, music, dance and drama.
On the basis of inheriting Chinese excellent traditional culture, we should also attach importance to cultural innovation. We often say "old country, new life". The so-called "old country and new life" is mainly embodied in respecting and carrying forward the tradition without following it, but adapting to the pace of the times and innovating traditional things. To build a strong socialist culture, we should also constantly bring forth the old and bring forth the new, thus enriching the content of Chinese culture. There are many ways of cultural innovation, one of which is the creative transformation and innovative development of Chinese excellent traditional culture. For example, Confucianism contains the humanistic spirit of people-oriented, the spirit of unremitting struggle for self-improvement, the patriotic spirit of loyalty to the country, and the spirit of unity of knowing and doing. For these spirits, we should carry out creative transformation and innovative development according to the requirements of the development of the times, and enrich the spiritual world of contemporary Chinese. We should also inject new factors into the ethics of Chinese excellent traditional culture to adapt it to modern society. Cultural innovation should also be based on today’s reality, adapt to the higher spiritual and cultural needs of the people in the new era, accelerate the development of cultural undertakings and cultural industries, and provide more excellent cultural products for the people.
The second is the relationship between bringing in and going out. Bringing in and going out are opposite and complementary, and they should develop in a balanced way. The purpose of introduction is to absorb the outstanding cultural achievements of all countries in the world and better develop Chinese culture; The purpose of going abroad is to let people all over the world know and understand Chinese culture and enhance its influence and appeal in the world. Comrade Supreme Leader emphasized that "civilizations are colorful because of communication, and civilizations are enriched because of mutual learning", and "we should all adopt the attitude of learning from and actively absorb the beneficial elements of various civilizations created by human society". Chinese culture emphasizes eclecticism and all rivers run into the sea. To build a strong socialist cultural country, it is necessary to introduce excellent cultural achievements from other countries and nations. It should be emphasized that the introduction of outstanding cultural achievements should not be swallowed up, let alone copied blindly, but should be reformed and innovated according to China’s national conditions to make it more suitable for China society.
To build a strong socialist cultural country, we should not only pay attention to importing, but also pay attention to going abroad. Only by making Chinese culture have an important influence in the world can China be regarded as a cultural power. Chinese excellent traditional culture has had a profound influence on many countries, including western countries. From the 17th century to the 18th century, some western missionaries translated and introduced some classic works of ancient China to European countries, which shocked the ideological circles of many European countries and formed an upsurge of worshipping China culture. The revolutionary culture and advanced socialist culture created by the Communist Party of China (CPC), who led the people of China after the founding of the People’s Republic of China, have become a powerful spiritual driving force for the development of China, and the spirit of China has attracted worldwide attention. Nowadays, people are more and more aware that Chinese culture contains important enlightenment to solve the problems faced by contemporary mankind. Therefore, Chinese culture is facing rare opportunities and broad space to go global. To promote Chinese culture to go abroad, first, it can increase the export of cultural products; Second, we can enlarge and strengthen the mainstream media, broaden the channels of communication and improve the communication power of Chinese culture; Third, we can strengthen foreign cultural exchanges; Fourth, it can support foreign Chinese education and Chinese culture education.
The third is the relationship between unity and diversity. The Chinese nation has formed a common spiritual home in the long-term historical development process, and worships the same mainstream values and ethics, which makes Chinese culture unified. But Chinese culture has the characteristics of diversity. As the saying goes: "A hundred miles of different winds, a thousand miles of different customs." China has a vast territory and many ethnic groups, and different ethnic groups and regions have their own cultural characteristics, which makes Chinese culture show diversity. The unity and diversity of culture are not simple opposites, but the relationship between generality and individuality. Cultural unity is a universal attribute of cultures of all ethnic groups and regions; Cultural diversity reflects the uniqueness of cultures of all ethnic groups and regions.
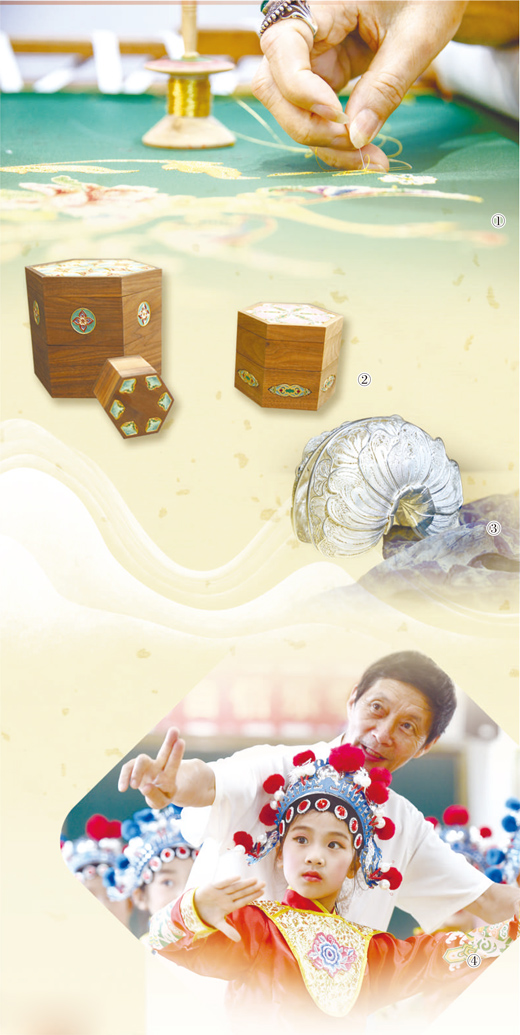
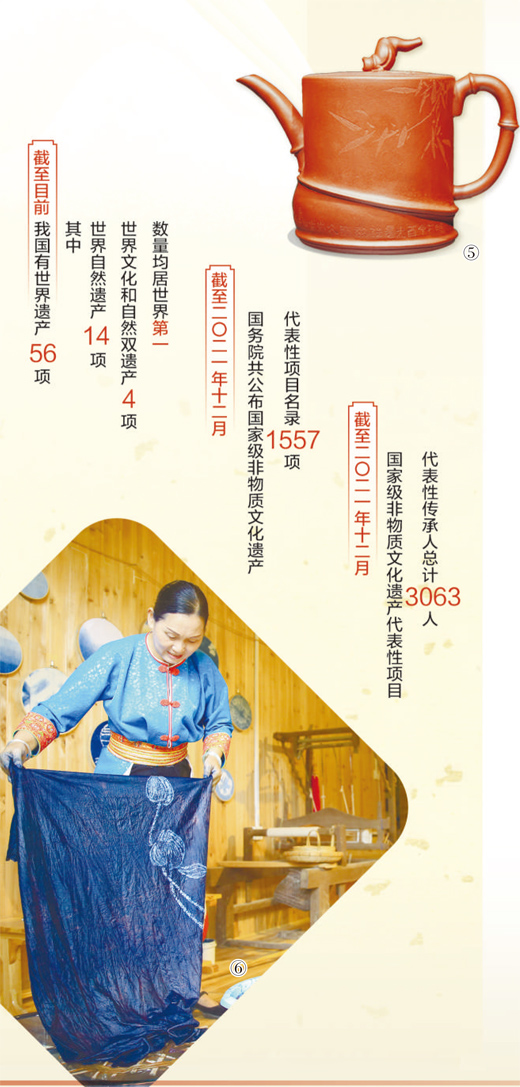
The key to enhancing cultural unity is to cultivate and practice socialist core values in the whole society. The socialist core values are the concentrated expression of contemporary China spirit, which embodies the common value pursuit of all the people. It is necessary to give play to the leading role of socialist core values in national education, the creation of spiritual civilization and the creation, production and dissemination of spiritual and cultural products, and integrate socialist core values into all aspects of social development. To protect cultural diversity, an important task is to protect and inherit the performing arts such as music, dance, drama, folk art, acrobatics and other handicrafts such as carving, embroidery, knitting and dyeing of all ethnic groups and regions, as well as to protect all kinds of life etiquette, New Year’s festivals and ethnic medicines.
(The author is a member of the Chinese Academy of Social Sciences and a counselor of the State Council)
The only way for the modern transformation of Chinese excellent traditional culture
"Two Innovations": the Scientific Policy of Building a Cultural Power (Seeking Truth from the Situation)
Li Zonggui
Contemporary China is striding forward on the road of socialist modernization. In the new journey of building a socialist modern power in an all-round way, how to make Chinese excellent traditional culture glow in the Spring Festival, help develop Socialism with Chinese characteristics culture and provide spiritual nourishment for building a spiritual home shared by the Chinese nation is a realistic problem to be solved urgently in building a socialist cultural power. In recent years, the Supreme Leader has clearly put forward and repeatedly stressed that it is necessary to promote the creative transformation and innovative development of Chinese excellent traditional culture. "Two Innovations" is the full expression of cultural self-confidence and self-consciousness, the basic principle and the only way to promote the transformation of Chinese excellent traditional culture from tradition to modernity, the scientific policy for us to treat Chinese excellent traditional culture correctly and build a socialist cultural power, and the important guarantee for creating new glory of Chinese culture.
Creative transformation and innovative development are the organic unity of inheritance and innovation. First of all, it emphasizes that Chinese excellent traditional culture has modern value and is a historical and cultural resource worthy of our serious exploration and vigorous promotion. Since the 18th National Congress of the Communist Party of China, the Supreme Leader has made many important expositions on the value of Chinese excellent traditional culture. He emphasized: "Chinese culture has a long history, accumulating the deepest spiritual pursuit of the Chinese nation, representing the unique spiritual identity of the Chinese nation, and providing rich nourishment for the endless development and growth of the Chinese nation." The report of the 19th National Congress of the Communist Party of China clearly pointed out that Socialism with Chinese characteristics culture originated from the excellent traditional Chinese culture nurtured by the 5,000-year civilization history of the Chinese nation, was cast in the revolutionary culture and advanced socialist culture created by the party leading the people in revolution, construction and reform, and was rooted in the great practice of Socialism with Chinese characteristics. This important thesis emphasizes that Socialism with Chinese characteristics culture originates from Chinese excellent traditional culture, which is a full affirmation of Chinese excellent traditional culture, a cultural consciousness of adhering to Chinese cultural position and inheriting Chinese context, and also the fundamental reason for us to promote the creative transformation and innovative development of Chinese excellent traditional culture.
Creative transformation and innovative development is a scientific attitude towards Chinese excellent traditional culture, which not only requires us to respect and inherit Chinese excellent traditional culture, but also is good at transforming and developing Chinese excellent traditional culture. Marxist philosophy tells us that dialectical negation is sublation, reservation, abandonment and transformation. For Chinese traditional culture, including the excellent traditional culture, it is obviously historical nihilism to completely deny it, but it will turn into revivalism to completely copy it. Promoting the creative transformation and innovative development of Chinese excellent traditional culture requires us to adhere to the guidance of Marxism, to carry forward the excellent cultural spirit that spans time and space, transcends the country, has eternal charm and has contemporary value under the guidance of the national spirit with patriotism as the core and the spirit of the times with reform and innovation as the core, so as to adapt Chinese excellent traditional culture to contemporary culture, coordinate with modern society and constantly glow with new vitality to nourish the spiritual world of contemporary Chinese. No matter from the theory of cultural development or from the practice of cultural development, the policy of "two innovations" is a strategic policy to treat Chinese excellent traditional culture scientifically and develop Socialism with Chinese characteristics culture under the new era conditions, and it is a transcendence and innovation of various traditional cultures in the past, which is of great significance to building a socialist cultural power.
To promote the creative transformation and innovative development of Chinese excellent traditional culture, the premise is to have an objective and rational value evaluation of Chinese excellent traditional culture. This kind of value evaluation should not only rely on sentiment, intuition and subjective feelings, but also form a scientific value evaluation standard according to the needs of Socialism with Chinese characteristics’s development in the new era and the great rejuvenation of the Chinese nation. The excellent Chinese traditional culture that we want to creatively transform and develop should be beneficial to governing the country, social development, moral construction, cultural identity, national unity, national rejuvenation and the development of world civilization. It is good to have some of these qualities, but it is precious to have only one. Among them, it includes core ideas, such as caring, attaching importance to people-oriented, keeping honesty, advocating justice, respecting harmony and seeking great harmony; It also includes Chinese traditional virtues, such as self-improvement, respect for career and happiness, helping the poor, being brave, filial piety and loving relatives; It also includes the Chinese humanistic spirit, such as the enlightenment thought of carrying Tao by literature and educating people by culture, the aesthetic pursuit of combining form and spirit with scene, and the life concept of frugality, neutrality and harmony.
Socialism with Chinese characteristics’s remarkable achievements since the reform and opening up cannot be separated from the encouragement of China spirit. In the new era, to develop Socialism with Chinese characteristics’s culture and build a socialist cultural power, we must further build the spirit of China and hold high the spirit of China. Promoting the creative transformation and innovative development of Chinese excellent traditional culture is an important way to build the spirit of China. As long as we adhere to the policy of "two innovations", we can constantly use the outstanding cultural achievements created by the Chinese nation to educate people with culture, provide spiritual guidance for the people, and provide spiritual impetus for the development of Socialism with Chinese characteristics.
(The author is a professor of philosophy at Sun Yat-sen University and a special researcher at Socialism with Chinese characteristics Thought Research Center, the supreme leader of Guangdong Province.)
Constantly create new glory of Chinese culture.
Grasp the basic requirements of developing Socialism with Chinese characteristics culture (seeking truth from the situation)
Gao changwu
The report of the 19th National Congress of the Communist Party of China pointed out: "To develop Socialism with Chinese characteristics culture is to take Marxism as a guide, adhere to the Chinese cultural stance, base on the reality of contemporary China and combine the conditions of the present era to develop a national, scientific and popular socialist culture facing modernization, the world and the future, and promote the coordinated development of socialist spiritual civilization and material civilization." This important exposition clarifies the basic requirements for developing Socialism with Chinese characteristics culture and building a socialist cultural power: taking Marxism as the guide, adhering to the position of Chinese culture, basing on the reality of contemporary China and combining the conditions of the present era. Only by thoroughly implementing these basic requirements can we promote the prosperity of socialist culture and build a strong socialist culture.
Guided by Marxism. Marxism creatively reveals the development law of human society, is a scientific world outlook and methodology, and is a powerful ideological weapon for people to know the world, grasp the law, pursue the truth and transform the world. Marxism is the fundamental guiding ideology for building the party and the country, and it is also the fundamental guiding ideology for promoting cultural construction. The report of the 19th National Congress of the Communist Party of China made strategic arrangements for promoting socialist cultural construction, including firmly grasping the leadership of ideological work, cultivating and practicing socialist core values, strengthening ideological and moral construction, prospering and developing socialist literature and art, and promoting the development of cultural undertakings and cultural industries. No matter what kind of work, we must always adhere to Marxism as the guidance. For example, if we want to firmly grasp the leadership of ideological work, we must consolidate the guiding position of Marxism in the ideological field, promote the modernization and popularization of Marxism in China, build a socialist ideology with strong cohesion and leading power, and unite all the people closely in ideals, beliefs, values and moral concepts. Practice has fully proved that only by adhering to the guidance of Marxism can cultural construction always maintain the correct direction and provide a strong spiritual force for the development of the cause of the party and the people. In the new era, to develop Socialism with Chinese characteristics culture and build a socialist cultural power, we must take a clear-cut stand on the fundamental issue of adhering to Marxism, and we must not waver at any time or under any circumstances. If we give up the guidance of Marxism, cultural construction will lose its direction and even go astray.
Stick to the position of Chinese culture. Socialism with Chinese characteristics culture is a culture with distinctive China characteristics, China style and China style. The reason for this is that it is deeply rooted in the rich and profound fertile soil of Chinese excellent traditional culture, deeply rooted in Socialism with Chinese characteristics’s great practice, and embodies a distinct Chinese cultural stand. Adhering to the position of Chinese culture is an inevitable requirement for the development of Socialism with Chinese characteristics culture, and it is also a fundamental requirement for Socialism with Chinese characteristics culture to gain a firm foothold and have important influence in the world cultural agitation. To adhere to the position of Chinese culture, we must first strengthen cultural self-confidence. Comrade Supreme Leader pointed out: "Cultural self-confidence is a more basic, deeper and more lasting force." Without firm cultural self-confidence, it is impossible to truly adhere to the position of Chinese culture. We should embody our firm cultural self-confidence and stick to the Chinese cultural stance in all aspects of building a socialist cultural power, and let the world know the cultural spirit, cultural pursuit and cultural responsibility of the Chinese nation.
Based on the reality of contemporary China. Contemporary China reality belongs to the category of objective reality and social existence, while Socialism with Chinese characteristics culture belongs to the category of subjective understanding and social consciousness. Marxism holds that social existence determines social consciousness. Therefore, the development of Socialism with Chinese characteristics culture must be based on the reality of contemporary China. Based on the reality of contemporary China, the key is to deeply understand that Socialism with Chinese characteristics has entered a new era. To develop Socialism with Chinese characteristics culture and build a socialist cultural power, we must base ourselves on the new era, a new historical orientation of China’s development, fully reflect the development of Socialism with Chinese characteristics in the new era, and strive to meet the higher requirements of the people in the new era for spiritual and cultural life. Based on the reality of contemporary China, through cultural construction, the world can better understand "developing China", "opening China" and "China contributing to human civilization".
Combined with the conditions of today’s times. In today’s era, the world is in a period of great development, great change and great adjustment, and world multipolarization, economic globalization, social informatization and cultural diversity are developing in depth. At the same time, the instability and uncertainty facing the world are increasingly prominent, and mankind faces many common challenges. As far as cultural development is concerned, all kinds of ideas and cultures in the world are stirring with each other, exchanges and encounters are more frequent, and the strategic position of culture in the competition of comprehensive national strength is further highlighted. However, some western developed countries use the long-standing advantage of cultural discourse power to infiltrate the developing countries in an attempt to maintain the old world cultural pattern through "cultural hegemonism". At the same time, scientific and technological progress and the rise of cultural industries have provided new opportunities for cultural development. To build a strong socialist cultural country, we must combine the current conditions of the times, profoundly grasp the cultural development trend, and make Socialism with Chinese characteristics culture always reflect the spirit and requirements of the times.
(Author: Central Party History and Literature Research Institute)